Imagine paying $350 for a month’s supply of insulin. Now imagine getting the exact same therapeutic result for $25. This isn’t a hypothetical scenario; it is the reality for millions of patients who switch to generic drugs. In the complex world of health economics, few mechanisms drive down costs as effectively as generic competition. While brand-name medications grab headlines with their high price tags and marketing budgets, generics quietly handle the heavy lifting of keeping healthcare affordable.
In 2024, generics accounted for 90% of all prescriptions filled in the United States-roughly 3.9 billion scripts. Yet, they represented only 12% of total prescription drug spending. Brand-name drugs, making up just 10% of prescriptions, consumed 88% of the market’s financial resources. This stark disparity highlights why understanding the role of generics is essential for anyone interested in controlling healthcare costs.
The Economic Engine: How Generics Slash Prices
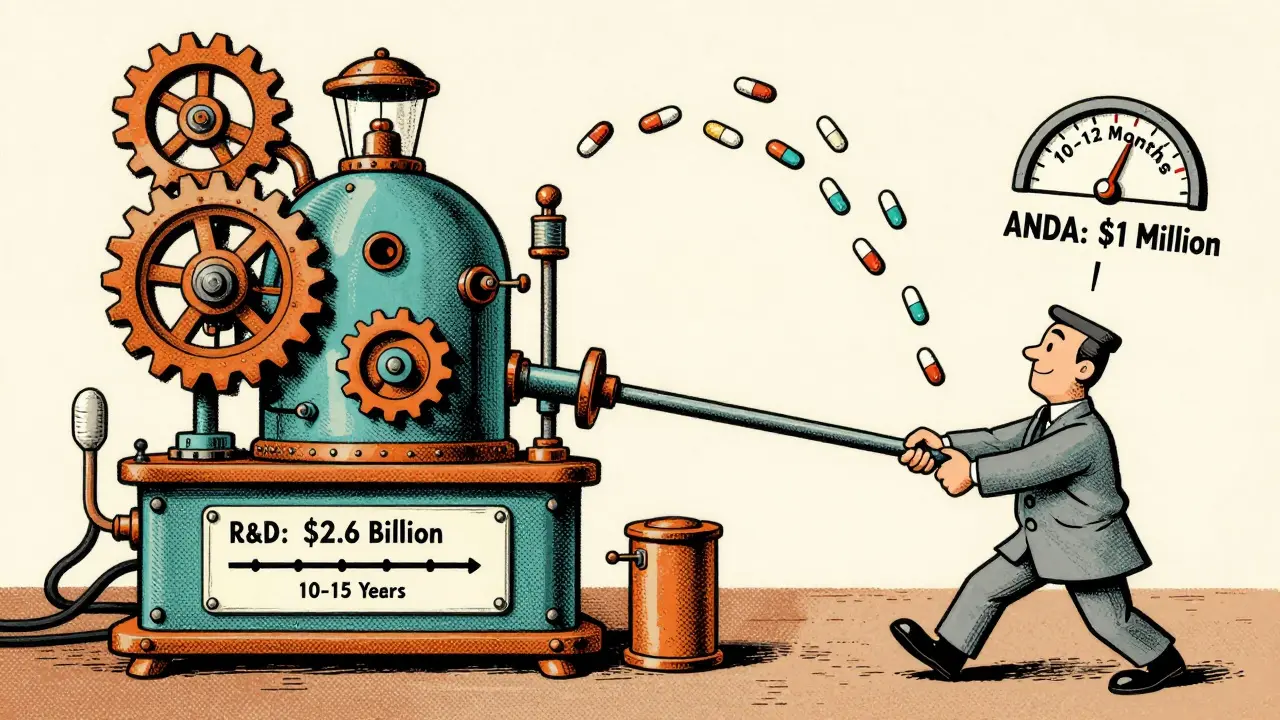
To understand why generics are so cheap, you have to look at what goes into making them. When a pharmaceutical company develops a new brand-name drug, it spends billions on research, clinical trials, and regulatory approval. These costs can take 10 to 15 years and average around $2.6 billion per successful drug. To recoup this investment, companies hold patents that grant them exclusive rights to sell the medication for a set period.
Once those patents expire, other manufacturers can step in. They don’t need to repeat the expensive clinical trials. Instead, they submit an Abbreviated New Drug Application (ANDA) to the Food and Drug Administration (FDA). This process typically takes 10 to 12 months and costs about $1 million-a fraction of the original development expense. Because these competitors aren’t paying for initial research, they can offer the drug at a significantly lower price. On average, generics cost 80-85% less than their brand-name counterparts.
| Factor | Brand-Name Drug | Generic Drug |
|---|---|---|
| Development Time | 10-15 years | 10-12 months |
| Average Cost | $2.6 billion | $1 million |
| Clinical Trials Required | Full Phase I-III trials | Bioequivalence studies only |
| Price Reduction Impact | N/A (Reference Price) | 80-85% lower |
This price drop isn’t just nice to have; it’s critical for system sustainability. The Congressional Budget Office estimates that generic competition reduces drug prices by 90% within one year of patent expiration. For context, Medicare negotiation scenarios might achieve a 42% reduction. That difference matters when you’re looking at national healthcare budgets.
Safety and Efficacy: Are Generics Really Equivalent?
A common concern among patients is whether cheaper means inferior. The short answer is no. By law, generic drugs must be bioequivalent to the brand-name version. This means they contain the same active ingredient, strength, dosage form, and route of administration. The FDA requires rigorous testing to ensure that the generic drug performs similarly in the body to the reference product.
Specifically, the FDA looks at pharmacokinetic parameters like Cmax (maximum concentration) and AUC (area under the curve). The 90% confidence intervals for these metrics must fall within 80-125% of the brand-name drug’s values. If a generic passes this test, it is considered therapeutically equivalent. You can check this status using the FDA’s Orange Book, which lists over 14,000 approved generic products. Products with an 'A' code indicate no known bioequivalence problems, giving prescribers and pharmacists confidence in substitution.
However, there are nuances. Inactive ingredients-the fillers, binders, and dyes-can differ between brands and generics. While these don’t affect the drug’s primary action, some patients report sensitivity to certain fillers. An FDA MedWatch report from 2023 noted 1,247 adverse event reports related to generic substitutions, primarily involving gastrointestinal issues due to different excipients. For most people, this is not an issue, but it’s a valid consideration for those with specific allergies or sensitivities.
The Biosimilar Frontier: Complex Molecules and Biologics
While small-molecule generics dominate the volume of prescriptions, a growing segment of healthcare spending comes from biologic drugs. These are large, complex molecules derived from living organisms, used to treat conditions like cancer, rheumatoid arthritis, and Crohn’s disease. Because of their complexity, they cannot be exactly copied like traditional pills. Instead, we have biosimilars, which are highly similar versions of reference biologics.
Biosimilars face a steeper regulatory hurdle. They require more extensive analytical methods and sometimes clinical testing to demonstrate similarity. As a result, their development costs are 30-40% higher than standard generics. Consequently, the discount they offer is smaller-typically 15-35% compared to the reference biologic. However, given the high list prices of biologics, even a modest percentage cut translates to significant savings.
The challenge here is adoption. In Europe, biosimilar adoption rates hover between 70-85%. In the U.S., they lag behind at 25-30%. Why? Pharmacy Benefit Managers (PBMs) often structure formularies to favor brand-name drugs if the rebates they receive offset the higher list price. This creates a "biosimilar void," where despite being available, these cost-effective alternatives aren’t reaching enough patients. Addressing this gap is crucial because specialty drugs account for 51% of total drug spending despite representing only 5% of prescriptions.
Barriers to Entry: Patents, Litigation, and Supply Chains
If generics are so effective at lowering costs, why don’t we see them immediately after a patent expires? The answer lies in strategic delays. Brand manufacturers employ various tactics to extend market exclusivity. One common method is the "patent thicket," where companies file dozens-or even hundreds-of secondary patents covering everything from formulation to manufacturing processes. The Federal Trade Commission found that brand manufacturers file an average of 140+ patents per drug.
Another tactic is "product hopping." Just before a patent is set to expire, a company might introduce a slightly modified version of the drug-perhaps a different dosage form or delivery mechanism-and shift marketing efforts to the new version. This forces generic makers to start the approval process over for the new formulation, delaying competition by 6-12 months or more.
Then there’s the issue of supply chain vulnerability. During the pandemic, shortages exposed the fragility of generic drug supplies. About 80% of Active Pharmaceutical Ingredients (APIs) are manufactured overseas, primarily in India and China. When disruptions occur, generics are disproportionately affected because margins are thin, leaving little buffer for inventory buildup. In 2023, the FDA identified 127 drugs at risk of shortage due to manufacturing quality issues, highlighting the need for domestic resilience.

Real-World Impact: Patient Stories and Systemic Savings
The numbers tell one story, but patient experiences bring it home. Consider the case of insulin. Before recent interventions, many patients paid hundreds of dollars monthly for brand-name insulin. With the introduction of generic insulin lispro and policy changes capping costs at $35/month for Medicare beneficiaries, thousands avoided rationing doses. A GoodRx report from 2024 showed that 68% of patients skipped doses or split pills when generics weren’t available. Switching to a generic option didn’t just save money; it improved adherence and health outcomes.
On a systemic level, the savings are staggering. Cumulative savings from generics reached $445 billion in 2023 alone. These funds free up resources for other areas of healthcare, from preventive care to hospital infrastructure. For employers, lower drug costs mean reduced premiums. For governments, it means slower growth in public health expenditures. It’s a win-win that relies entirely on robust generic competition.
Looking Ahead: Policy and Future Trends
The landscape is evolving. The Inflation Reduction Act has introduced Medicare drug price negotiations, aiming to cap costs for high-spending drugs. While this will save billions, experts argue it complements rather than replaces generic competition. Negotiation works best for drugs without generic alternatives. For off-patent drugs, generic substitution remains the most powerful tool.
Future projections suggest prescription medicine use will continue to rise, driven by an aging population. IQVIA forecasts 215 billion days of therapy in 2024. To manage this demand sustainably, we need to address the barriers mentioned earlier. Streamlining ANDA approvals, cracking down on anti-competitive practices, and incentivizing biosimilar development are key steps. Additionally, promoting transparency in PBM rebate structures could help direct patients toward truly cost-effective options.
As we move forward, the role of generics will only become more central. They are not just a budgetary line item; they are a cornerstone of accessible healthcare. Understanding their value helps us advocate for policies that keep medicines affordable and available for everyone.
Are generic drugs as safe and effective as brand-name drugs?
Yes. The FDA requires generic drugs to be bioequivalent to brand-name drugs, meaning they must deliver the same amount of active ingredient into your bloodstream in the same amount of time. They undergo rigorous testing to ensure safety, purity, and potency are identical. While inactive ingredients may vary, they do not affect the drug's therapeutic effect for the vast majority of patients.
Why are generic drugs so much cheaper than brand-name drugs?
Generic drugs are cheaper because manufacturers do not incur the high costs of initial research and development, such as clinical trials. Once a brand-name drug’s patent expires, generic companies can produce the same medication using existing data, submitting only an Abbreviated New Drug Application (ANDA). This significantly lowers production and regulatory costs, allowing for substantial price reductions, typically 80-85% lower than the brand name.
What is the difference between a generic drug and a biosimilar?
Generic drugs are copies of small-molecule chemical drugs, while biosimilars are copies of large, complex biological molecules produced in living cells. Because biologics are more complex, they cannot be exact duplicates; instead, biosimilars are "highly similar" to the reference product with no clinically meaningful differences in safety, purity, or potency. Biosimilars typically offer smaller discounts (15-35%) compared to generics (80-85%).
Can my pharmacist automatically substitute a brand-name drug with a generic?
In most cases, yes. Forty-eight states allow pharmacists to automatically substitute a generic for a brand-name drug if the prescriber does not explicitly forbid it. However, for narrow therapeutic index drugs (like warfarin or levothyroxine), some states require explicit prescriber authorization. Always check with your pharmacist or doctor if you have concerns about switching.
Why are there sometimes shortages of generic drugs?
Generic drug shortages often stem from supply chain vulnerabilities. Since margins are low, manufacturers may operate with minimal inventory buffers. Additionally, a significant portion of Active Pharmaceutical Ingredients (APIs) is sourced from overseas, primarily India and China. Disruptions in manufacturing, quality control issues, or geopolitical events can lead to shortages, affecting multiple suppliers simultaneously.
Do insurance plans prefer generic drugs?
Generally, yes. Most insurance plans, including Medicare Part D, encourage generic use through lower copays. Ninety-eight percent of Medicare Part D plans automatically substitute generics when available. However, in commercial plans, Pharmacy Benefit Managers (PBMs) may sometimes steer patients toward brand-name drugs if rebates make them financially advantageous for the plan, despite higher list prices.