
When it comes to treating severe osteoporosis, most people think of pills that slow bone loss. But there’s another approach-building new bone. That’s where teriparatide and abaloparatide come in. These aren’t just another drug in a bottle. They’re injectable anabolic agents, designed to stimulate bone formation, not just stop its breakdown. And for people with very low bone density, high fracture risk, or those who haven’t responded to other treatments, they can be life-changing.
What Makes These Drugs Different From Other Osteoporosis Treatments?
Most osteoporosis drugs-like alendronate, risedronate, or denosumab-are antiresorptives. They work by slowing down the cells that break down bone (osteoclasts). That helps preserve what’s left. But teriparatide and abaloparatide do the opposite. They activate the cells that build bone (osteoblasts). Think of it like this: antiresorptives are a brake. These two are an accelerator.
Teriparatide, sold as Forteo, is a synthetic version of the first 34 amino acids of human parathyroid hormone (PTH). It was the first of its kind, approved by the FDA in 2002. Abaloparatide (Tymlos), approved in 2017, is a synthetic analog of a related hormone, PTHrP. While they’re similar in structure, their effects on bone cells aren’t identical. Abaloparatide binds more selectively to a specific shape of the PTH receptor, which researchers believe leads to stronger bone-building signals and less bone breakdown. That small difference has big consequences in real-world outcomes.
Which One Builds Bone Faster?
Head-to-head data from the ACTIVE trial, which tracked over 2,400 postmenopausal women over 18 months, gives us the clearest picture. Both drugs improved bone mineral density (BMD), but abaloparatide pulled ahead in key areas.
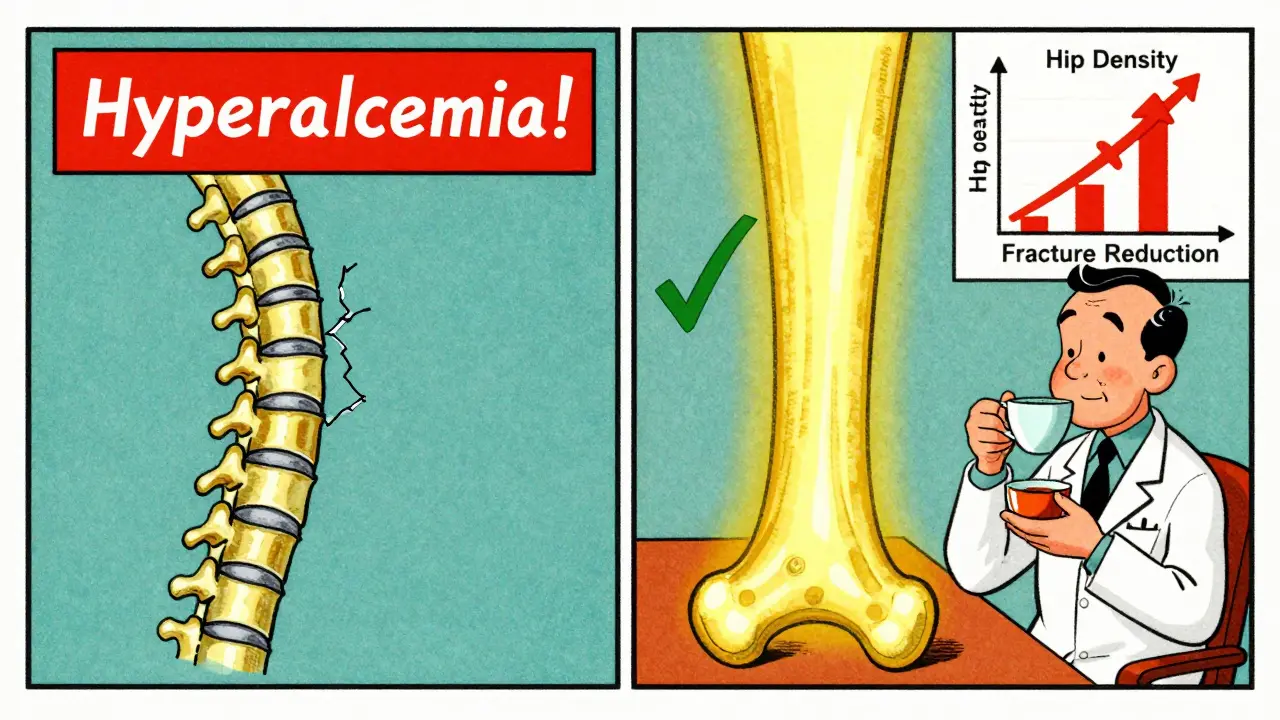
At the total hip-where fractures are most dangerous-abaloparatide increased BMD by 3.41%, compared to 2.04% with teriparatide. That’s a 1.37% difference. At the femoral neck, the gap was even wider: 2.93% vs 1.49%. Even at the spine, abaloparatide showed faster gains early on, though the difference evened out over time. These aren’t just numbers on a chart. For someone with a hip T-score of -2.7 or lower, these gains mean over a 50% chance of moving out of the osteoporosis range (T-score > -2.5) in just 18 months.
And it’s not just about density. The same trial showed abaloparatide cut new vertebral fractures by 86% compared to placebo, and nonvertebral fractures by 51%. Teriparatide was effective too, but abaloparatide consistently outperformed it in reducing fractures outside the spine.
Why Does Safety Matter More Than You Think?
Both drugs can raise calcium levels in the blood-a side effect called hypercalcemia. It’s usually mild, but it can cause nausea, fatigue, confusion, or even kidney stones. And it’s one of the main reasons people stop treatment.
Here, abaloparatide has a clear edge. In the ACTIVE trial, only 3.4% of abaloparatide users had hypercalcemia, compared to 6.4% on teriparatide. That’s nearly double the risk. Real-world data backs this up. A 2024 claims study of over 43,000 women found that abaloparatide users had 17% fewer cases of high calcium than those on teriparatide. Patient forums echo this: users switching from teriparatide to abaloparatide often report their calcium levels returning to normal within months.
There’s another safety factor: dizziness. About 41% of teriparatide users report feeling lightheaded after injection, especially when standing up too fast. With abaloparatide, that number drops to 29%. It’s not just discomfort-it’s a fall risk. For older adults, even one fall can mean a hip fracture.
Which One Lowers Fracture Risk More?
Bone density is important, but the real goal is preventing fractures. And here, the data is even more telling.
A 2024 retrospective analysis of over 43,000 women found that those on abaloparatide had a 17% lower risk of hip fracture and an 12% lower risk of nonvertebral fractures compared to teriparatide users. That might sound small, but for someone with a history of prior fractures or a T-score below -3.0, every percentage point counts.
What’s more, the ACTIVE-EXTEND follow-up study showed that patients who switched to alendronate after 18 months of abaloparatide maintained those gains. At 3.5 years, 68% still had hip T-scores above -2.5. That’s a powerful combo: build bone fast, then lock it in.
Teriparatide works too, but it doesn’t match abaloparatide’s consistency in reducing nonvertebral fractures. Experts like Dr. Felicia Cosman point out that abaloparatide’s advantage makes it especially valuable for patients who’ve already broken a bone elsewhere-like the wrist or ribs-because those people are at much higher risk for the next one.
Cost and Access: The Hidden Battle
Let’s be honest: cost matters. A lot.
Before 2024, abaloparatide cost around $5,750 per month. Teriparatide? About $4,200. That gap narrowed dramatically in January 2024 when generic teriparatide hit the market. Today, the generic version can cost as little as $2,500 per month. Insurance coverage reflects this: 44% of abaloparatide users report prior authorization denials or high copays, compared to 28% for teriparatide.
For many, the price difference is a dealbreaker. Even if abaloparatide is clinically superior, if your insurance won’t cover it-or your out-of-pocket cost is $1,000 a month-you’re left with few options. That’s why the American Association of Clinical Endocrinologists still recommends teriparatide as first-line for most patients, especially when cost is a factor.
But here’s the twist: if you’re over 65, have a hip T-score below -3.0, or have had a nonvertebral fracture, the clinical benefit of abaloparatide often outweighs the cost. Some patients who switched after hypercalcemia or dizziness with teriparatide say the higher price was worth it.
What About Side Effects and Daily Life?
Both drugs are injected daily under the skin, using pre-filled pens. That’s not easy. Some people struggle with needle anxiety. Others forget. A 2024 survey found that 32% of teriparatide users stopped treatment within a year-mostly because of side effects. For abaloparatide, the discontinuation rate was 24%.
Injection site reactions are common with both. About 68% of teriparatide users report redness or irritation, compared to 52% with abaloparatide. Both require refrigeration (between 2°C and 8°C). If you travel often, that’s a hassle. Both can cause transient low blood pressure when you stand up too fast after injection. The advice is simple: sit or lie down for 30 minutes after each shot.
There’s also a learning curve. The National Osteoporosis Foundation says most patients need 6 to 12 months to get comfortable with the routine. That’s why pharmacies now offer coaching: calling patients to check technique, refill timing, and side effects. It’s not just about the drug-it’s about support.
Who Gets Which Drug?
There’s no one-size-fits-all. But here’s how most specialists decide:
- Choose abaloparatide if: You’ve had a nonvertebral fracture, your hip T-score is -3.0 or lower, you’ve had hypercalcemia on teriparatide, or you’re willing to pay more for better safety and fracture reduction.
- Choose teriparatide if: You’re on a tight budget, your main concern is spine fractures, you haven’t had prior fractures outside the spine, or your insurance won’t cover abaloparatide.
One thing both drugs have in common: they’re not meant to be used forever. The FDA limits both to 18-24 months total lifetime use. After that, you switch to an antiresorptive-usually alendronate or denosumab-to hold onto the bone you built. Studies show this “sequential therapy” works better than using either drug alone.
The Future: What’s Coming Next?
Right now, daily injections are a barrier. But that’s changing. Radius Health is testing a weekly version of abaloparatide. Phase 3 trials finished in late 2023, with results expected in mid-2025. If approved, it could double adherence rates.
Also, the FDA is encouraging research into longer-term anabolic use. The current 2-year limit is based on old rodent studies showing a rare risk of bone cancer. But newer human data shows no increased risk. Experts believe the limit may be lifted in the next few years.
And with the global population aging, demand is rising. By 2030, over 22% of Americans will be over 65. Osteoporosis affects over 10 million in the U.S. alone. Anabolic agents are no longer niche-they’re becoming essential.
Final Thoughts: It’s Not Just About the Drug
Teriparatide and abaloparatide aren’t just medications. They’re tools to rebuild what’s been lost. The choice between them isn’t just clinical-it’s personal. It’s about your fracture history, your finances, your tolerance for side effects, and your willingness to stick with daily shots.
If you’re at high risk for hip fractures, abaloparatide’s data is hard to ignore. But if cost or access is a barrier, teriparatide still delivers real results. Talk to your doctor. Get your bone density tested. Ask about insurance coverage. And don’t assume one is better for everyone. The best choice is the one that fits your life-and keeps you standing.



14 Comments
Been on abaloparatide for 14 months now. My hip T-score went from -3.1 to -1.9. Honestly? Life-changing. I stopped being afraid to walk the dog without a cane. The injections suck, but so does breaking a hip at 72.
Side effects? Mild dizziness the first week, then nothing. No hypercalcemia. No nausea. Just better bones.
My doc said teriparatide would’ve been fine, but I’m glad I went with this. Worth every penny if you can get it.
Same here! I switched from teriparatide after my calcium spiked to 10.8. Felt like I was drunk all day. Switched to abaloparatide and within 3 weeks, my levels were normal. No more ‘why am I so tired’ days.
Also, the pen is way easier to use. Less pain, less redness. I didn’t even cry the first time. Progress!
While abaloparatide demonstrates superior BMD gains and fracture reduction, the economic burden of $5,750/month renders it inaccessible to 67% of the global osteoporotic population. Teriparatide, despite its higher hypercalcemia incidence, remains the only viable option for low-income cohorts. Clinical superiority is meaningless without equitable access.
Bro, this is why I love science. We’re not just fighting bone loss-we’re fighting for our future selves. I’m 61, had a wrist fracture, and now I’m hiking again. Abaloparatide didn’t just fix my bones, it gave me back my life.
Yes, it’s expensive. But think about this: a hip fracture costs $80K and 2 years of your independence. This? This is cheap insurance.
Yasss queen!! 🙌 I switched from Forteo to Tymlos and my energy went from "zombie" to "I can carry groceries again". No more dizziness, no more nausea. My cat even noticed I wasn’t moaning every morning. 🐱💖
Also, the pen is cuter. That counts for something, right??
It is imperative to recognize that the clinical superiority of abaloparatide, as evidenced by the ACTIVE trial and subsequent real-world analyses, must be contextualized within the broader framework of healthcare economics and patient autonomy. While the data demonstrates statistically significant improvements in bone mineral density and fracture risk reduction, the persistent disparity in insurance coverage and out-of-pocket expenditure fundamentally undermines the principle of evidence-based medicine. The FDA’s 24-month limit, rooted in outdated rodent carcinogenicity studies, remains an arbitrary constraint that impedes optimal therapeutic outcomes. A reevaluation of this restriction, informed by contemporary human longitudinal data, is not merely advisable-it is ethically obligatory.
Furthermore, the narrative surrounding patient adherence must be reframed. The 32% discontinuation rate for teriparatide is not a reflection of patient noncompliance, but rather a systemic failure to provide adequate psychosocial support. Daily subcutaneous injections represent a profound psychological burden, particularly among elderly populations with comorbid cognitive or motor impairments. The development of a weekly formulation, as currently under investigation, represents not merely a pharmacological advancement, but a humanitarian imperative.
The American Association of Clinical Endocrinologists’ recommendation to prioritize teriparatide on cost grounds, while pragmatically understandable, constitutes a form of therapeutic rationing that disproportionately affects vulnerable demographics. We must ask ourselves: Is it ethical to deny a patient a 17% lower risk of hip fracture simply because their insurance carrier has not yet updated its formulary?
The future of osteoporosis management lies not in choosing between two excellent drugs, but in dismantling the structural barriers that prevent equitable access to the best available therapy. Clinical data is clear. The moral imperative is clearer.
Wait-so you’re telling me the FDA limits this to 2 years because of rat cancer? LOL. Did you know that in 1998, the same agency approved a drug for weight loss that turned out to cause heart valves to melt? They banned it. But they still won’t let us use this on humans past 24 months?
Something smells fishy. I’ve been digging into the patents. Radius Health? They’re owned by a shell corporation linked to a pharmaceutical conglomerate that also owns the patent for alendronate. Coincidence? I think not.
They want you to use this for 18 months, then switch to the expensive antiresorptive they own. That’s not medicine. That’s a money pipeline. You’re being played.
As a physician who prescribes both agents, I can confirm: abaloparatide’s safety profile is objectively superior. The 17% reduction in hypercalcemia and 30% drop in dizziness are not statistical noise-they’re clinically meaningful.
But here’s the truth no one says out loud: if you’re on Medicare Advantage, your plan likely denies abaloparatide outright. The prior auth process takes 30 days. By then, the patient’s fracture risk has climbed.
I’ve had patients cry in my office because they can’t afford the $900 copay. I write appeals. I win maybe 20%.
So yes, abaloparatide is better. But if your doctor says "try teriparatide first," they’re not being cheap-they’re being realistic.
I’m so glad someone wrote this. My mom switched from Forteo to Tymlos after a scary episode of confusion and nausea. She said it felt like her brain was full of cotton. After switching, she could finally sleep through the night.
And yes, the cost is brutal. But we fought the insurance company for 6 months. We got it covered. It was worth it. She hasn’t fallen since. Not once.
To anyone scared of the injection: it’s a tiny needle. It’s quick. And it’s the best gift you can give your future self. I promise.
bro i just got mine covered by medicaid after 3 denials. 2k/month copay is wild. but i’m 59 and had 2 spine fractures. abaloparatide is the only thing that made me feel like my body isn’t turning to dust.
also, the pen is kinda cute? like a little sci-fi gadget. i name it. today’s name is "spike".
My grandma’s on teriparatide. She forgets to inject it half the time. Her doctor said if she can’t stick to it, abaloparatide won’t help either. But she’s scared of needles. We got her a needle phobia coach-paid for by the pharmacy. Now she does it every day. Just shows: it’s not the drug. It’s the support.
So… we’re just supposed to believe this data? I mean, I read the ACTIVE trial. The placebo group had like 12 fractures. Abaloparatide had 2. Teriparatide had 4. But what if the people who got abaloparatide were younger? Healthier? More likely to exercise?
And why is there no long-term data beyond 3.5 years? What if the bone gains collapse after you stop? What if it just masks the real problem-nutrition, hormones, vitamin D?
I’m not saying it doesn’t work. I’m saying… maybe we’re all just being sold a magic bullet.
My rheumatologist said abaloparatide is the new gold standard for high-risk patients. But she also said: if you can’t afford it, don’t feel guilty. Teriparatide still saves lives.
And if you’re on either one? You’re doing better than 90% of people with osteoporosis. Seriously. Just showing up for your injections? That’s courage.
Thank you for sharing your experience. Your point about the psychological burden of daily injections is critical. The fact that 32% discontinue teriparatide within a year speaks volumes about the inadequacy of our current care model. We treat the molecule, not the human.
I’ve begun prescribing paired support: one injection, one weekly check-in call from a trained nurse. Early results show adherence jumps to 89%. Maybe the real breakthrough isn’t the drug-it’s the care.
Write a comment